Neonatal hypoglycemia is a condition marked by low blood glucose levels in newborns, often occurring within the first few hours of life as they adapt from a glucose-rich intrauterine environment. While transient hypoglycemia can be part of a newborn's natural adaptation, prolonged or severe hypoglycemia requires prompt intervention to prevent potential neurological harm. Here’s an in-depth look at the risk factors, management strategies, and approaches to support breastfeeding while treating hypoglycemia in newborns, based on the Academy of Breastfeeding Medicine's Protocol #1.
Risk Factors for Neonatal Hypoglycemia
Certain maternal and neonatal conditions can increase the likelihood of hypoglycemia, necessitating glucose monitoring and possibly proactive management. Key risk factors include:
- Maternal Diabetes: Both gestational and pre-existing diabetes can predispose the infant to hyperinsulinemia, leading to rapid declines in blood glucose after birth.
- Intrauterine Growth Restriction (IUGR) and Low Birth Weight: Infants with limited glycogen and fat stores may struggle with glucose regulation.
- Prematurity: Immature metabolic systems make preterm infants more susceptible to glucose instability.
- Perinatal Stress: Conditions like hypoxia or cold stress can increase glucose utilization, pushing the infant towards hypoglycemia.
- Large for Gestational Age (LGA): Infants of mothers without diabetes but who are LGA may also experience hypoglycemia due to high insulin levels.
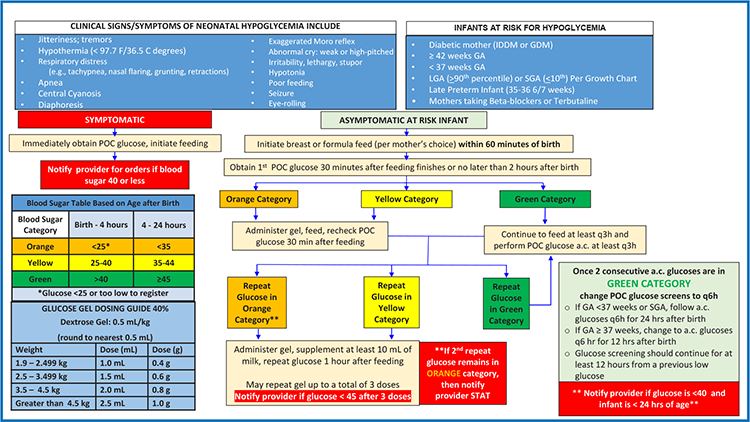
Symptoms of Hypoglycemia in a Newborn
In newborns, hypoglycemia can present with a variety of symptoms. These can be subtle and are sometimes challenging to detect, especially in asymptomatic cases. According to the Academy of Breastfeeding Medicine’s Protocol #1, here are the key symptoms:
- Jitteriness or tremors
- Irritability
- Pallor (pale skin) or vasomotor instability
- Tachypnea (rapid breathing)
- Tachycardia (rapid heart rate)
- Temperature instability or hypothermia
- Sweating (less common in newborns)
- Exaggerated Moro reflex (startle reflex)
- Lethargy or listlessness
- Hypotonia (reduced muscle tone, appearing limp)
- Poor feeding or refusal to feed
- Apnea (pauses in breathing) or irregular breathing
- Seizures
- Coma (in severe cases)
Additional Signs
Newborns may also exhibit:
- Cyanosis (bluish skin coloration due to lack of oxygen)
- High-pitched crying
- Weak suck or poor feeding coordination
Since these symptoms are non-specific and may overlap with other neonatal issues, prompt blood glucose testing in at-risk infants is critical to confirm hypoglycemia and initiate appropriate treatment
Balancing Hypoglycemia Treatment with Breastfeeding Support
Effective management involves balancing blood glucose stabilization with the preservation of breastfeeding, as early interruption can disrupt lactation establishment. Here are evidence-based approaches to support breastfeeding during hypoglycemia management:
- Early Skin-to-Skin and Breastfeeding: Initiating skin-to-skin contact immediately after birth and encouraging breastfeeding within the first hour help regulate newborn blood glucose. Breastfeeding provides small but frequent doses of colostrum, ideal for supporting early metabolic needs.
- Using Dextrose Gel as a First-Line Treatment: For mild hypoglycemia, 40% dextrose gel applied buccally has been shown to stabilize blood glucose without requiring separation from the mother. This method supports breastfeeding continuity and can be safely combined with breastfeeding to boost blood glucose levels further. According to the protocol, dextrose gel can effectively prevent NICU admissions and reduce the need for formula supplementation.
- Frequent Blood Glucose Monitoring: For at-risk infants, monitoring should begin within the first few hours and continue before feedings until stable glucose levels are achieved. This avoids unnecessary interventions and supports breastfeeding by allowing time for natural metabolic adjustment. Persistent or severe hypoglycemia, particularly if blood glucose is below 20–25 mg/dL, may require intravenous glucose therapy, but breastfeeding can resume as soon as the infant is stabilized.
- Avoiding Routine Supplementation: Routine formula supplementation can interfere with breastfeeding and delay milk supply establishment. Instead, if additional feeding is required, expressed colostrum or pasteurized donor milk is preferred to protect the breastfeeding process.
Protocols for Hypoglycemia Treatment and Breastfeeding
The Academy of Breastfeeding Medicine emphasizes that maintaining the breastfeeding relationship is critical during hypoglycemia treatment. Following their guidelines:
- Mild to Moderate Hypoglycemia: Use glucose gel alongside breastfeeding. This combination has been shown to be effective in stabilizing blood glucose while supporting breastfeeding success.
- Severe or Persistent Hypoglycemia: If glucose levels remain low or the infant shows severe symptoms (e.g., seizures, altered consciousness), IV glucose therapy may be required. In these cases, breastfeeding should continue during IV therapy to minimize separation and to support milk production.
Source: Florida Pediatrician — Neonatal Hypoglycemia Management
Supporting Parents and Alleviating Concerns
Managing neonatal hypoglycemia while prioritizing breastfeeding requires a collaborative approach and clear communication with parents. Educating them on the safety of their breast milk, the temporary nature of supplementation, and the importance of frequent breastfeeding helps to alleviate anxiety and empowers them to stay engaged in their infant’s care.
Protecting Breastfeeding
- Hand Express to collect colostrum if baby is unwilling to breastfeed for a feeding or two.
- Feed expressed colostrum via spoon, cup, or syringe.
- Begin pumping if baby is unwilling or unable to breastfeed more than twice.
- Encourage mom to pump every 3 hours for 15 minutes with 2 minutes of hand expression following pumping until baby is able to successfully breastfeed for every feeding.
Effective hypoglycemia management in the breastfed newborn involves monitoring glucose levels, recognizing risk factors, and intervening thoughtfully to protect both infant health and breastfeeding. By incorporating dextrose gel and encouraging early skin-to-skin contact and breastfeeding, healthcare providers can support glucose stabilization without compromising lactation, allowing for a healthier start for both mother and baby.
References
Academy of Breastfeeding Medicine. (2022). Protocol #1: Guidelines for Glucose Monitoring and Treatment of Hypoglycemia in Term and Late Preterm Neonates. Breastfeeding Medicine, 17(3), 1-10.
Hoermann, H., Roeper, M., Dafsari, R. S., Koestner, F., Schneble, D., von Zezschwitz, D., Mayatepek, E., Kummer, S., & Meissner, T. (2022). Protecting against brain damage by improving treatment in neonates with hypoglycaemia: ProBrain-D—a study protocol of a prospective longitudinal study. BMJ Open, 12(e063009). https://doi.org/10.1136/bmjopen-2022-063009